
N-acetylcysteine (NAC) is a precursor to reduced glutathione, and both of these play important roles in health and fitness. NAC has a long history of use as a first-aid remedy for acetaminophen (known as paracetamol in Europe) poisoning.
It’s given in cases when you’ve taken an overdose of Tylenol or other acetaminophen products. It neutralizes the toxic effects of the drug by recharging glutathione, thereby preventing liver damage.
NAC and glutathione may also be important in COVID-19, as explained by pulmonologist Dr. Roger Seheult in the MedCram lectures above. The reason for this is because of the role they play in combating oxidative stress, which is a main cause of inflammation and disease in general, and the cytokine storm associated with COVID-19 in particular. NAC may also combat the abnormal blood clotting seen in many cases.
Biochemistry Primer
As explained and illustrated by Seheult, when you add an electron to an oxygen (O2) molecule, you get superoxide (O2), a reactive oxygen species (ROS). When you add another electron (for a total of two electrons), you get hydrogen peroxide (H2O2). An oxygen molecule with three electrons added becomes hydroxyl (O3), and oxygen with four electrons added becomes water (H2O).
Oxygen is the most oxidized form, while water is the most reduced form. Your body has built-in defenses against oxidative stress like1 superoxide dismutase (SOD). SOD converts damaging superoxide into hydrogen peroxide. Another is catalase, which converts hydrogen peroxide into oxygen and water. A third is glutathione peroxidase (GSHPX).
GSHPX does two things simultaneously. While reducing hydrogen peroxide into water, it also converts the reduced form of glutathione (GSH) into glutathione disulfide (GSSG), which is the oxidized form of glutathione. In other words, as GSHPX turns hydrogen peroxide into harmless water, glutathione becomes oxidized.
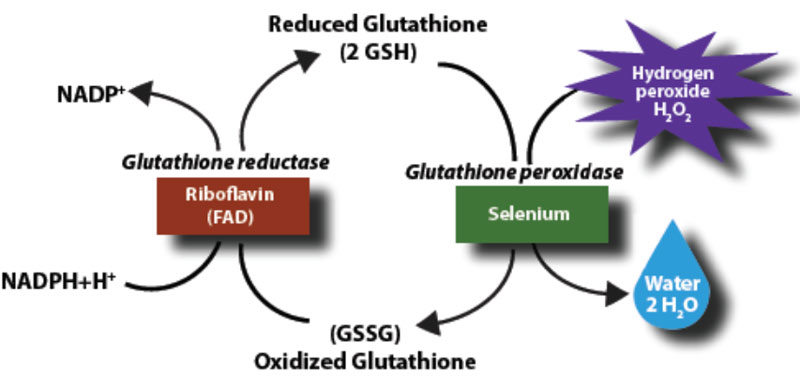
The oxidized GSSG is then “recharged” or regenerated by NADPH (the reduced form of NADP+), turning it back into GSH (the reduced form of glutathione). NADPH is also converted into NADP+ through an enzyme called GSH reductase.
The reason this is important is because superoxide plays a crucial role in the oxidative stress occurring in the chronic illnesses identified as comorbidities for COVID-19, such as obesity, heart disease and diabetes.
As noted by Seheult, serious COVID-19 infection triggers a perfect storm of superoxide-driven oxidative stress, as SARS-CoV-2 attaches to the ACE2 receptor, triggering angiotensin 2 (AT-2), which stimulates superoxide. Simultaneously, there’s a deficiency of AT-1,7, which inhibits superoxide. So, this deficiency allows superoxide to accumulate further.
SARS-CoV-2 also attracts polymorphonuclear leukocytes (PMNs), a type of white blood cell, which also produces superoxide in its efforts to destroy pathogens. All of that superoxide is then converted into other ROS that destroy endothelial cells.
This down-spiral can be inhibited by N-acetylcysteine (NAC), which boosts GSSG. As illustrated by Seheult, when you add two GSH molecules and hydrogen peroxide together, you end up with oxidized glutathione and harmless water, thus alleviating the oxidative stress.
NAC Boosts GSH and Protects Against Influenza
Seheult cites research showing low GSH and oxidative stress are associated with a range of nose, ear and throat conditions, affecting tissues both locally and systemically. The good news is that glutathione can be recharged with NAC, an inexpensive and readily available over-the-counter supplement.
Research2 has in fact demonstrated that NAC can attenuate symptoms of influenza and improve cell-mediated immunity. According to the authors:
“N-acetylcysteine (NAC), an analogue and precursor of reduced glutathione, has been in clinical use for more than 30 yrs as a mucolytic drug. It has also been proposed for and/or used in the therapy and/or prevention of several respiratory diseases and of diseases involving an oxidative stress, in general.
The objective of the present study was to evaluate the effect of long-term treatment with NAC on influenza and influenza-like episodes. A total of 262 subjects of both sexes … were enrolled in a randomized, double-blind trial … randomized to receive either placebo or NAC tablets (600 mg) twice daily for 6 months.
Patients suffering from chronic respiratory diseases were not eligible, to avoid possible confounding by an effect of NAC on respiratory symptoms. NAC treatment was well tolerated and resulted in a significant decrease in the frequency of influenza-like episodes, severity, and length of time confined to bed.
Both local and systemic symptoms were sharply and significantly reduced in the NAC group. Frequency of seroconversion towards A/H1N1 Singapore 6/86 influenza virus was similar in the two groups, but only 25% of virus-infected subjects under NAC treatment developed a symptomatic form, versus 79% in the placebo group …
Administration of N-acetylcysteine during the winter, thus, appears to provide a significant attenuation of influenza and influenza-like episodes, especially in elderly high-risk individuals. N-acetylcysteine did not prevent A/H1N1 virus influenza infection but significantly reduced the incidence of clinically apparent disease.”
NAC Is a Potent Antiviral in Its Own Right
As noted by Seheult, the number needed to treat (NNT) in that study3 is 0.5, which means for every two people treated with NAC, one will be protected against symptomatic influenza. (Remember, you can be infected with a virus yet not become ill, i.e., symptomatic, if your immune system is strong enough.)
That’s significantly better than influenza vaccines, which have an NNT, or NNV (number needed to vaccinate) of 71,4 meaning 71 people must be vaccinated to prevent a single case of confirmed influenza. It’s even better than vitamin D, which has an NNT of 33.5 (Among those who were severely vitamin D deficient at baseline, taking vitamin D still had an NNT of 4.)
NAC has also been shown to inhibit viral replication and expression of pro-inflammatory cytokines, such as interleukin-6 (IL-6), in cells infected with highly pathogenic H5N1 influenza virus.6 According to the authors:
“The antiviral and anti-inflammatory mechanisms of NAC included inhibition of activation of oxidant sensitive pathways including transcription factor NF-kappaB and mitogen activated protein kinase p38 …
NAC inhibits H5N1 replication and H5N1-induced production of pro-inflammatory molecules. Therefore, antioxidants like NAC represent a potential additional treatment option that could be considered in the case of an influenza A virus pandemic.”
NAC in Acute Respiratory Distress Syndrome
NAC has also been shown to reduce acute respiratory distress syndrome (ARDS),7 which is a serious complication associated with acute lung injury (ALI). One meta-analysis8 of five randomized controlled trials found a significant reduction in intensive care unit (ICU) stays among patients treated with NAC, even though there was no significant difference in short-term mortality risk.
Another earlier study9 found NAC improves ARDS by “increasing intracellular glutathione and extracellular thiol molecules” along with general antioxidant effects. According to this study:
“In acute respiratory distress syndrome (ARDS), there is extensive overproduction of free radicals to the extent that endogenous antioxidants are overwhelmed, permitting oxidative cell damage.
The present study examined the benefit of the anti-oxidant compound N-acetylcysteine (NAC) in the management of ARDS by measuring patient’s intracellular glutathione (inside red blood cells) and extracellular (plasma) anti-oxidant defense biomarkers and outcome.
Twenty-seven ARDS patients were recruited from the intensive care unit of a teaching Hospital and randomly divided into two groups. Both groups were managed similarly by regular treatments but 17 patients received NAC 150 mg/kg at the first day that followed by 50 mg/kg/day for three days and 10 patients did not receive NAC.
Treatment by NAC increased extracellular total anti-oxidant power and total thiol molecules and also improved intracellular glutathione and the outcome of the patients. In conclusion, patients with ARDS are in a deficient oxidant-anti-oxidant balance that can get a significant benefit if supplemented with NAC.”
NAC Improves Lung Function
Other studies that have shown NAC to be beneficial in the treatment of lung-related problems include the following:
• A 1994 study10 found NAC enhances recovery from ALI, significantly regressing patients’ lung injury score during the first 10 days of treatment, and significantly reducing the need for ventilation.
After three days of treatment, only 17% of those receiving NAC needed ventilation, compared to 48% in the placebo group. According to the authors:
“Intravenous NAC treatment during 72 h improved systemic oxygenation and reduced the need for ventilatory support in patients presenting with mild-to-moderate acute lung injury subsequent to a variety of underlying diseases.”
• A 2018 study11 found NAC reduces oxidative and inflammatory damage in patients with community-acquired pneumonia.
• Another 2018 study12 found NAC also improves post-operative lung function in patients undergoing liver transplantation.
NAC Protects Against Blood Clots and Stroke
Importantly, with regard to COVID-19, NAC may protect against the coagulation problems associated with this illness. Many COVID-19 patients experience serious blood clots, and NAC counteracts hypercoagulation in the blood as well.13,14,15
As noted in one of these studies,16 “NAC has anticoagulant and platelet-inhibiting properties.” Another study points out that:17
“… diabetes exacerbates stroke-induced brain injury, and that this correlates with brain methylglyoxal (MG)-to-glutathione (GSH) status. Cerebral injury was reversed by N-acetylcysteine (NAC).
Here we tested if the pro-thrombotic phenotype seen in the systemic circulation and brain during diabetes was associated with increased MG-glycation of proteins, and if NAC could reverse this …
NAC treatment partly or completely reversed the effects of diabetes. Collectively, these results show that the diabetic blood and brain become progressively more susceptible to platelet activation and thrombosis.
NAC, given after the establishment of diabetes, may offer protection against the risk for stroke by altering both systemic and vascular prothrombotic responses via enhancing platelet GSH, and GSH-dependent MG elimination, as well as correcting levels of antioxidants such as SOD1 and GPx-1.”
A fourth paper,18 published in 2017, found NAC has potent thrombolytic effects, meaning it breaks down blood clots. The authors concluded that “NAC is an effective and safe alternative to currently available antithrombotic agents to restore vessel patency after arterial occlusion.” (Restoring vessel patency means the blood vessel is now unobstructed so that blood can flow freely.)
Seheult cites two additional papers19,20 showing the same thing. As noted by Seheult, many COVID-19 cases have blood clots in addition to excessive oxidative stress, and NAC addresses both of these problems.
NAC for COVID-19
Last but not least, a report21 reviewing the evidence for using NAC in the treatment of COVID-19 was published April 14, 2020, by The Centre for Evidence-Based Medicine at the University of Oxford.
This report focuses on acute respiratory disorders, and we now know that COVID-19 is not just a respiratory disorder but also a blood disorder. This is a significant shortcoming of this report, as there’s significant evidence that NAC can break down the blood clots responsible for the hypoxia (cellular deprivation of oxygen) in COVID-19.
May 5, 2020, a trial was posted to ClinicalTrials.gov, for the study of NAC in patients with COVID-19, sponsored by the Memorial Sloan Kettering Cancer Center.22 The study aims to enroll 86 patients with severe or critical illness to investigate whether NAC, in addition to other supportive treatments, can reduce ICU stays and prevent the need for mechanical ventilation. Here, they are giving 6 grams (6,000 milligrams) of NAC a day for up to three weeks.
Seheult’s hypothesis for why NAC may be useful in COVID-19 treatment can be summarized as follows:
SARS-CoV-2 attaches to and reduces the ACE2 receptor, which causes AT-2 to increase and AT-1,7 to decrease. This in turn increases damaging superoxide that causes oxidative stress and endothelial cell dysfunction.
This then increases von Willebrand factor from the endothelial space, causing thrombosis (blood clots), and it is this thrombosis that appears to cause the hypoxia in the lungs. NAC — which recharges glutathione — not only reduces superoxide (oxidative stress) but also appears to reduce von Willebrand factors that form blood clots.
Glutathione for COVID-19
In the second MedCram video (second in the playlist), Seheult reviews the blood clotting aspects of COVID-19. He also discusses the potential effectiveness of simply taking glutathione, opposed to its precursor, NAC.
A recent case report23 — which simply reviews one or more medical cases and is not an actual study — reports that two patients with COVID-19 and a history of Lyme disease (coinfection) treated with 2 grams of intravenous glutathione “improved their dyspnea within one hour of use.” Dyspnea is the medical term for shortness of breath. According to the authors:
“Oral and IV glutathione, glutathione precursors (N-acetyl-cysteine) and alpha lipoic acid may represent a novel treatment approach for blocking NF-κB and addressing ‘cytokine storm syndrome’ and respiratory distress in patients with COVID-19 pneumonia.”
He also cites a Russian paper24 stating that glutathione deficiency may be “the most likely cause of serious manifestation and death” in COVID-19 patients. The paper, which is a preprint and has not yet undergone peer review, presents a hypothesis “based on an exhaustive literature analysis and own observations.” According to the author:25
“The major risk factors established for severe COVID-19 infection and relative glutathione deficiency found in COVID-19-infected patients with moderate-to-severe illness have converged me to two very important conclusions:
(1) oxidative stress contributes to hyper-inflammation of the lung leading to adverse disease outcomes such as acute respiratory distress syndrome, multiorgan failure and death;
(2) poor antioxidant defense due to endogenous glutathione deficiency as a result of decreased biosynthesis and/or increased depletion of GSH is the most probable cause of increased oxidative damage of the lung, regardless which of the factors aging, chronic disease comorbidity, smoking or some others were responsible for this deficit.
The hypothesis provides novel insights into the etiology and mechanisms responsible for serious manifestations of COVID-19 infection and justifies promising opportunities for effective treatment and prevention of the illness through glutathione recovering with N-acetylcysteine and reduced glutathione.”
As noted by Seheult, we still do not have any trials demonstrating that NAC will benefit COVID-19 patients specifically, “but if we connect the dots, it looks promising.” What’s more, NAC is very safe and many studies have shown there are no serious adverse effects associated with its use.
The same can be said for glutathione. Seheult points out it would be interesting to see what the effect might be using a combination of both glutathione and NAC. Overall, the more we learn about this disease, the more we realize there may be simple and inexpensive ways to treat this perplexing illness, and NAC in particular looks like a good candidate for consideration.
Of course, both also have many other important health benefits. To learn more, see “Glutathione and NAC Play Crucial Roles in Health and Fitness,” and “The Many Benefits of NAC — One of the Most Important Supplements You’ve Likely Never Heard Of.”